泌尿时讯 发表时间:2025/12/31 18:24:21
编者按:前列腺癌是男性常见的恶性肿瘤之一;尽管前列腺特异性抗原(PSA)监测依然是早期发现BCR的重要手段,但随着影像学进步和ARPI研究的公布以及立体定向放疗的发展,根治性前列腺切除术后高危生化复发(BCR)患者的诊治理念和手段都有了较大改变。在近期举行的ESMO大会上,EMBARK研究公布了总生存数据,进一步证实了恩扎卢胺为高危BCR患者带来的生存获益。肿瘤瞭望-泌尿时讯特邀卡罗莱纳州泌尿学研究中心医学主任Neal D. Shore教授分享EMBARK研究背景及数据,以及对未来临床实践影响等精彩内容。
01
《肿瘤瞭望-泌尿时讯》:EMBARK研究分析了恩扎卢胺联合方案在高危BCR前列腺癌中的获益数据,能否分享下相关研究背景及其对于前列腺癌的早期干预的价值?
Neal D. Shore教授:大约11年前,当我们首次设计EMBARK试验时,已经有了一些很有参考价值的早期数据。这些数据主要涉及那些在接受前列腺切除术、前列腺放疗,或者在前列腺切除术后又接受了辅助放疗,随后出现生化复发(也就是PSA复发)的患者。从这些数据中我们发现,如果患者的PSA倍增时间非常缓慢(如达到12个月以上),特别是患者的传统影像学检查结果为阴性时,我们可以对这些患者进行密切监测。要知道,在11年前,我们的检测手段还比较有限,主要是依靠CT扫描和传统的骨扫描。
与此同时,我们已经看到了口服雄激素受体通路抑制剂(例如恩扎卢胺)的显著疗效。在《新英格兰医学杂志》发表的AFFIRM和PREVAIL两项重要试验表明,对于化疗失败以及化疗前的转移性去势抵抗性前列腺癌(mCRPC)患者来说,与仅使用雄激素剥夺疗法(ADT)相比,联合使用ARPI能带来明确的额外获益。
基于这些发现,我们不禁思考,既然mCRPC患者能从ADT+ARPI的治疗中获益,那么如果我们把这种治疗方法提前应用到疾病更早期的阶段,又会发生什么呢?其实在此之前,我们已经在非转移性去势抵抗性前列腺癌(nmCRPC)领域开展了相关研究,像PROSPER试验,还有更早一些由我负责领导的STRIVE试验等,在这些试验中我们都看到了治疗获益。而且,我们从早期分析(主要来自约翰霍普金斯大学的研究)中了解到,那些在前列腺切除术或放疗后病情复发,并且PSA倍增时间非常快(短于9个月)的患者,发展成影像学可见转移的可能性更大。所以,我们针对生化复发且PSA倍增时间小于等于9个月的患者设计了这项研究。
这项研究设置了三个不同的队列,第一个队列采用的是传统的LHRH激动剂加上安慰剂的治疗方法。第二个队列的治疗方案是LHRH联合恩扎卢胺,第三个队列则是单独使用恩扎卢胺进行治疗,并且采用开放标签,研究主要终点是无转移生存期(MFS)。我们在2023年的美国泌尿外科学会(AUA)年会上首次公布了初步信息,结果显示与单独使用LHRH治疗相比,联合治疗组的风险比(HR)约为0.4;而恩扎卢胺单药治疗对比LHRH单药治疗的HR约为0.65。在当时,总生存期(OS)方面也显示出了有获益的趋势,不过还没有达到统计学上的显著意义。
相关研究成果发表于《新英格兰医学杂志》,随后欧洲药品管理局(EMA)和美国食品药品监督管理局(FDA)等监管机构批准了恩扎卢胺用于治疗高危生化复发患者的扩展人群,但在药物标签中并没有具体说明“高危”含义。而通过对欧洲队列进行进一步的分析,目前在欧洲大部分地区,PSA倍增时间少于12个月被认定为高危生化复发的定义。
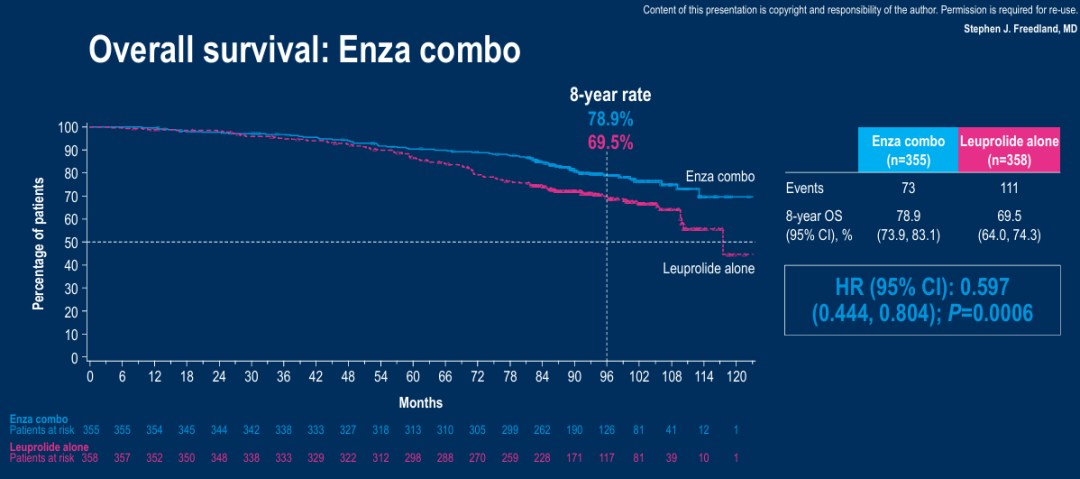
在2025年德国柏林举行的欧洲肿瘤内科学会(ESMO)年会上,我们公布了后续的随访数据,也就是长达8年的总生存随访结果。结果证实,恩扎卢胺联合LHRH治疗组在总生存期获益方面要优于LHRH单药治疗组,风险比为0.597。然而,恩扎卢胺单药治疗组与LHRH单药治疗组的总生存结果虽然没有达到统计学上的显著差异,但同样呈现出总生存获益的趋势。
Oncology Frontier- UroStream: The EMBARK study analyzed the benefit data of enzalutamide combination therapy in high-risk BCR prostate cancer. Could you share the relevant research background and its value for early intervention in prostate cancer?
Dr. Neal D. Shore:Eleven years ago, when we first designed the EMBARK trial, we had some very informative early data about patients who experienced biochemical relapse, or PSA recurrence, after undergoing prostatectomy, radiation therapy to the prostate, or both. Our data clearly indicated that if the PSA doubling time was quite slow, specifically over 10 to 12 months, we could safely monitor these patients, especially if they were negative on conventional imaging. Back then, our just only tools for imaging were CT scans and traditional bone scans.
At that time, we were already aware of the benefits of oral androgen receptor inhibitors, such as enzalutamide, from trials like AFFIRM and PREVAIL, which were published in the New England Journal of Medicine. These studies showed that adding an oral androgen receptor pathway inhibitor (ARPI) provided a clear additive benefit compared to just using androgen deprivation therapy (ADT) alone, whether it was post-chemotherapy mCRPC (AFFIRM) or pre-chemotherapy mCRPC (PREVAIL).
This led us to wonder: if testosterone suppression with ADT provides synergistic benefits, what would happen if we added an ARPI for patients with biochemical recurrence? We also had previous trials, like PROSPER, and others I was fortunate enough to lead, such as TERRAIN and STRIVE, which had shown promising signals of benefit. Additionally, earlier analyses, mostly from Johns Hopkins, revealed that patients who failed their initial treatment (prostatectomy or radiation) and had rapid PSA doubling times (less than 9 months) were much more likely to develop radiographic metastases. Therefore, we based our study design on patients with biochemical recurrence and a PSA doubling time of less than or equal to 9 months.
The trial included three cohorts. One cohort received traditional monotherapy with an LHRH agonist and a placebo. The main cohort compared LHRH plus enzalutamide against the control arm of LHRH plus placebo. A third cohort, which was open-label, received enzalutamide monotherapy without any sham placebo injections.
Here at ESMO 2025 in Berlin, Germany, we presented the 8-year follow-up data on overall survival. What we found was that the combination of enzalutamide and LHRH was superior to LHRH monotherapy, with a hazard ratio for overall survival benefit of 0.595. Looking at the overall survival follow-up for enzalutamide monotherapy versus LHRH monotherapy, while it was close, it did not reach statistical significance, although it still showed a trend towards a survival benefit.
02
《肿瘤瞭望-泌尿时讯》:基于这项研究及临床经验,是否会促使您对部分高危生化复发患者启动ARPI治疗,而不是像过去那样等待至出现影像学转移?在做出这个决策时,您会重点与患者沟通哪些利弊?
Neal D. Shore教授:不久前,我们的总生存数据在《新英格兰医学杂志》发表,相关成果也获得了众多同行认可。临床实践中,当与那些术后和(或)放疗后出现高危BCR的患者交流时,我充满信心。实际上,2025年ESMO大会的一项壁报研究显示,接受放疗的患者在恩扎卢胺单药治疗中获益尤为明显。
在临床上与高危生化复发的患者沟通治疗方案时,我已经不再对这些患者单独使用促黄体生成素释放激素(LHRH)激动剂或拮抗剂进行治疗,而是倾向于推荐恩扎卢胺的联合治疗方案,可以联合口服瑞卢戈利、注射地加瑞克或其他LHRH激动剂或拮抗剂等药物。不过有趣的是,这些患者中有不少人之前可能因为放疗等原因接受过ADT治疗,他们对那种治疗体验并不满意。例如,他们会出现严重的潮热、疲劳感等症状。而且我们知道,睾酮抑制不仅与心血管代谢综合征有关,还会导致骨质脱矿,对性功能也会产生明显影响,比如导致性欲减退或力比多丧失。
所以,当我告诉患者“我们可以试试恩扎卢胺单药治疗”时,他们都表现出浓厚的兴趣。这是因为根据发表在《新英格兰医学杂志》的患者报告结局数据显示,接受恩扎卢胺单药治疗的患者性欲有所改善,部分患者的勃起功能也会变得更好。同时,由于他们的睾酮和雌激素水平没有降低,所以骨质脱矿的情况肯定会减少。在认知方面,其影响似乎也有所改善或减轻。因此我经常通过共同决策的方式,为患者提供他们最感兴趣的治疗策略。
我在恩扎卢胺单药治疗试验中曾遇到过一些挑战,就是我们缺乏应对乳房相关增大、乳头触痛或疼痛等问题的策略。这一问题在EMBARK试验以及II期ENACT试验中均未被纳入考虑。在这两项研究中我们都发现,如果不采取任何措施来缓解因恩扎卢胺单药治疗导致的雌激素和睾酮水平升高所带来的影响,就会出现乳房增大(男性乳房发育症),可能还会伴有乳头触痛或疼痛。就像我们在大剂量比卡鲁胺的经验中所看到的那样。现在对于这类患者,可以采用低剂量的他莫昔芬(隔日10 mg),对于减轻乳房相关症状有所帮助。此外,也可以进行预防性乳房放疗,给予8到10戈瑞(Gray)的剂量,通常可以在一天内完成。
综上所述,从临床获益的角度来看,目前对于高危生化复发患者的标准治疗方法是ADT联合恩扎卢胺。不过针对某些特定患者,我也会和他们一起探讨恩扎卢胺单药治疗的可能性。
Oncology Frontier- UroStream: Based on this study and your clinical experience, would you initiate ARPI therapy in some patients with high-risk biochemical recurrence, rather than waiting until radiographic metastases develop, as has been the case in the past? What are the key pros and cons you discuss with your patients when making this decision?
Dr. Neal D. Shore:Our overall survival data were recently published in the New England Journal of Medicine, and the findings have been widely recognized by our peers. In clinical practice, I am confident when communicating with patients who develop a high-risk BCR after surgery and/or radiotherapy. In fact, a poster study presented at the 2025 ESMO Congress showed that patients receiving radiotherapy benefited significantly from enzalutamide monotherapy.
When I tell my patients that they could try enzalutamide monotherapy, they are very interested. In the data we have reviewed and published in New England Journal Evidence, patients on monotherapy enzalutamide have improved libido, some have better erectile function, certainly less bone demineralization due to the absence of testosterone and estrogen loss. There seems to be even some improvement or lessening of cognitive effects, although this can still be an issue since enzalutamide crosses the blood-brain barrier.
So yes, in response to your question, I believe that the standard of care for patients with high-risk biochemical recurrence, based on clinical benefits, is combination testosterone suppression therapies and enzalutamide. And for some patients, I review with them the option for enzalutamide monotherapy.
03
《肿瘤瞭望-泌尿时讯》:根据现有数据,哪些特征的高危生化复发患者(例如,特定的PSA倍增时间、初始 Gleason 评分)从恩扎卢胺治疗中获得的绝对生存获益最大?我们应如何利用生物标志物进行精准患者筛选?
Neal D. Shore教授:在EMBARK试验中,我们严格执行了PSA倍增时间≤9个月的入组标准。后续分析显示,即便患者的PSA倍增时间<12个月,他们也能从联合治疗或者恩扎卢胺单药治疗中取得相似获益。而对于PSA倍增时间>12个月的患者,我选择先观察而暂不进行治疗,因为我认为此时治疗风险大于获益。对于PSA倍增时间确切≤9个月以及部分<12个月的患者,我肯定会为他们提供联合治疗与恩扎卢胺单药治疗这两种选择。
目前出现了一些在EMBARK试验期间没有的新进展,那就是PSMA PET成像技术。当时我们所有患者在传统影像学检查上都是阴性,所以将他们定义为nmHSPC。如今,随着更先进的PSMA PET成像技术的应用,如果发现一个、两个、三个病灶,或许有人会认为只要少于五个,就有机会进行转移灶导向治疗。不过,目前还没有来自精心设计的III期试验的I级证据来支持这一观点,但相关的试验正在推进。接下来的问题是,如果要对这些患者进行转移灶的立体定向放疗,这些患者是否能从短期使用恩扎卢胺和/或ADT治疗中获益呢?这些都是需要通过持续监测来寻找答案的重要问题。
此外,研究中在第37周中断给药,这是首批在研究中加入中断治疗环节的大型试验之一,我对此深感自豪。这样一来,患者就有了一段我们称之为“假期”的治疗中断期,很多患者都很喜欢这一点。实际上我们还在考虑,由于恩扎卢胺单药治疗的耐受性可能非常好,而且不会降低患者的睾酮水平,也许这些患者可以从连续治疗中获益,而不是像那些接受恩扎卢胺和ADT的患者一样,有很长一段时间(超过15-18个月)完全停止治疗,直到他们的PSA复发。
我认为未来还有更多的答案等待我们去探寻,也需要开展更多的研究。在此,我想鼓励我在中国的同行们,如果你们遇到PSA倍增时间在12个月或更短的高危BCR患者,并且打算开始治疗,可以考虑采用ADT联合恩扎卢胺,或者恩扎卢胺单药治疗的方式,并与患者一起评估双药联合与单药治疗的利弊。
Oncology Frontier- UroStream: Based on the available data, which characteristics of patients with high-risk biochemical recurrence (e.g., specific PSA doubling time, initial Gleason score) derive the greatest absolute survival benefit from enzalutamide treatment? How can we use biomarkers for precise patient selection?
Dr. Neal D. Shore:In the EMBARK trial, we were strict about enforcing a PSA doubling time of less than or equal to 9 months. Subsequent analyses have shown that even patients with a PSA doubling time of less than 12 months can benefit similarly from either combination therapy or enzalutamide monotherapy. For my patients with a PSA doubling time greater than 12 months, I simply monitor them without initiating treatment, as I don't believe the risk justifies the benefit. For those with a definitely shorter doubling time, less than 9 months, and some with less than 12 months, I absolutely offer them the choice between combination therapy and enzalutamide monotherapy.
One final thought: In the study, we implemented a dose interruption at 37 weeks, making it one of the first large trials to include an interruption period, of which I'm very proud. This allowed patients to have what we call a "holiday" from their therapy, which many truly enjoyed. Given that enzalutamide monotherapy can be so well-tolerated without lowering testosterone levels, we're contemplating whether continuous therapy might benefit these patients, unlike those who received both enzalutamide and androgen deprivation therapy. Those patients had a very long period, over 15 to 18 months, without any therapy until they experienced a PSA relapse.
So, I believe there are still more answers to come and more research to be done. It's crucial, and I would encourage all my colleagues in China who treat patients with high-risk biochemical recurrence (BCR), particularly those with a doubling time of 12 months or less, to consider combination androgen deprivation therapy and enzalutamide, or enzalutamide monotherapy, when initiating treatment. They should review with their patients the pros and cons of doublet versus single therapy.
04
《肿瘤瞭望-泌尿时讯》:对于后续仍出现转移的患者,早期在生化复发阶段使用ARPI,会如何影响其进入转移性去势抵抗性前列腺癌阶段后的后续治疗选择?是否存在交叉耐药的问题?
Neal D. Shore教授:在前列腺癌的治疗过程中,随着患者从一种治疗阶段发展到另一种,我们不得不担忧克隆演变以及耐药病理情况的出现。耐药性问题在治疗决策和方案是一个棘手的难题。
我非常支持在患者病情进展时,尽可能使用多种具有新作用机制的药物。我们知道,首次治疗往往是最佳时机,所以要重视前线强化治疗,同时让患者保持良好的生活质量。不过,当患者在接受了ADT和ARPI治疗后病情出现进展,并且产生了耐药,我并不太主张依次序贯使用另一种ARPI。当然,参加临床试验也是一种选择,但这取决于所在国家的情况以及有哪些可用药物。
对于ADT和ARPI治疗后发展为mCRPC的患者,可以选择紫杉烷类化疗;如果病灶主要是骨转移,还可以使用镭223等放射性药物。此外,还有放射性配体疗法,其基本是基于PSMA导向的策略。另外,如果患者存在HRR突变,那么口服PARP抑制剂治疗也可能是一个合适的选择。
Oncology Frontier- UroStream: For patients who subsequently develop metastases, how does early ARPI use at biochemical recurrence affect their subsequent treatment options after they progress to metastatic castration-resistant prostate cancer? Is there a concern about cross-resistance?
Dr. Neal D. Shore:When patients progress from one line of therapy to another, we are concerned about clonal evolution and the emergence of certain resistant pathologies. Resistance poses a significant challenge in our discussions on treatment sequencing.
I firmly believe that as patients progress, it's crucial to introduce therapies with novel mechanisms of action. As is often said, "The first shot is the best shot." Therefore, intensifying treatment upfront while ensuring opportunities for patients to maintain a good quality of life is essential. If interruption of treatment is feasible and can be carefully monitored, I consider it a positive approach. However, if patients develop resistant disease after receiving ADT and an ARPI, I am not a strong advocate for switching to another ARPI. Of course, clinical trials remain an option, but their availability depends on the country's healthcare system and available resources.
For first-line mCRPC treatment following progression from a doublet of ADT and ARPI, several options exist. Taxane-based chemotherapy may be considered. Additionally, radiopharmaceuticals such as radium could be suitable, particularly for bone-predominant disease. There's also an expanding field of radioligand therapies, primarily focused on PSMA-directed strategies. Furthermore, if the patient has an HRR mutation, they might be a good candidate for oral PARP inhibitor therapy.
Neal D Shore 教授
卡罗莱纳州泌尿学研究中心医学主任
美国癌症免疫治疗学会(SITC)膀胱癌指南委员会成员
膀胱癌倡导网络、枫树联盟和杜克全球健康研究所的理事会成员
大型泌尿外科集团协会(LUGPA)专科网络前列腺癌学院和膀胱/肾癌学院主席
Neal D. Shore教授已主持超过400项临床试验,主要研究方向为泌尿生殖系统肿瘤。他撰写或合著了超过350篇同行评审论文和众多书籍章节。他曾担任/现任Reviews in Urology, Urology Times, Chemotherapy Advisor, OncLive, PLOS ONE, Urology Practice, JUOP and World Journal of Urology, and he also serves as an editor of Everyday Urology-Oncology的编委。