泌尿时讯 发表时间:2025/4/8 17:38:42
编者按:目前ADT仍是mHSPC的基石方案,但长期应用可能会增加心血管事件风险。近期在EAU大会公布的STAMPEDE研究数据显示,二甲双胍联合ADT可使高容量转移性激素敏感性前列腺癌(mHSPC)患者总生存期延长10个月(HR=0.79),同时改善代谢指标:体重增幅较少(2.5 kg vs 4 kg)、代谢综合征发生率减少(4.9% vs 9.4%)。《肿瘤瞭望-泌尿时讯》特邀研究讲者、英国曼彻斯特大学泌尿外科临床高级讲师Ashwin Sachdeva现场分享精彩内容。
Ashwin Sachdeva:这是一个非常重要的问题。当前我们已认识到雄激素剥夺疗法,尤其与雄激素受体通路抑制剂联用时会显著提升心血管事件的发生风险,甚至可能导致心血管相关死亡事件。去年,我们的相关研究成果荣登《JAMA Oncology》杂志,明确指出在采用ADT联合ARPI的治疗方案时,心血管不良事件的风险可能会成倍增加。因而在肿瘤治疗过程中,不应仅仅将关注点聚焦于肿瘤控制,更应从患者整体健康状况的角度出发,高度重视包括骨骼健康和心血管健康在内的治疗相关毒副作用管理。
在实际临床工作中,我们会主动筛查患者的心血管风险因素,如高血压、糖尿病等基础疾病。针对这些高危人群,我们会采取更为积极的预防措施。具体而言,我们会运用β-受体阻滞剂或钙通道阻滞剂来有效控制血压,同时密切监测患者的血糖水平并及时进行干预,以确保血糖得到良好控制。长期来看,这些干预策略能够切实有效地降低心血管事件的发生率。在面对复杂病例时,我们通常会与心脏肿瘤科医生展开紧密合作;而在相对简单的病例中,则会与基层医疗团队协同合作,共同致力于降低治疗过程中的相关不良反应,以保障患者的治疗安全和生活质量。
UroStream:ADT is a cornerstone treatment for prostate cancer, but it may increase cardiovascular risk and non-prostate cancer-related death, etc. How do you deal with these side effects in clinical practice?
Dr. Ashwin Sachdeva:That’s an excellent and very important question. We now recognize that ADT—and especially when intensified with androgen receptor pathway inhibitors (ARPIs)—can significantly raise the risk of cardiovascular events and even cardiovascular-related mortality.
In fact, we published a paper in JAMA Oncology last year indicating that the risk of cardiovascular complications may double when an ARPI is added to ADT. This highlights the importance of managing patients not just for oncological outcomes but also taking a holistic approach that addresses treatment-related toxicities—particularly in areas like bone and cardiovascular health.
One clinical strategy involves proactively monitoring patients for cardiovascular risk factors, such as baseline hypertension or diabetes. In individuals with pre-existing risk, we take a more aggressive preventive approach. This may include the use of medications like beta-blockers or calcium channel blockers to manage hypertension, and careful monitoring for diabetes, with early intervention to maintain glycemic control.
Over the long term, these preventive strategies have been shown to reduce cardiovascular events. In more complex cases, we may collaborate closely with cardio-oncology specialists, while in less complicated situations, we work with community physicians to manage cardiovascular risk profiles and minimize adverse effects from treatment.
Ashwin Sachdeva:我们此次在EAU大会报告了STAMPEDE研究二甲双胍相关数据,聚焦于转移性激素敏感性前列腺癌(M1期)患者群体。研究共纳入约1800名受试者,随机接受标准治疗或标准治疗联合长期二甲双胍(针对转移性患者的特定治疗方案),主要终点为总生存期。本次分析着重关注二甲双胍对代谢的影响,这也是该项研究的关键次要终点。我们已于去年的ESMO大会上公布了总生存数据,显示在未经筛选的整体人群中,联合二甲双胍并未带来显著生存获益(HR为0.91,点击链接查看ESMO 2024研究结果:ESMO 2024丨二甲双胍联合ADT治疗,或可改善高容量mHSPC患者的预后和代谢情况)。
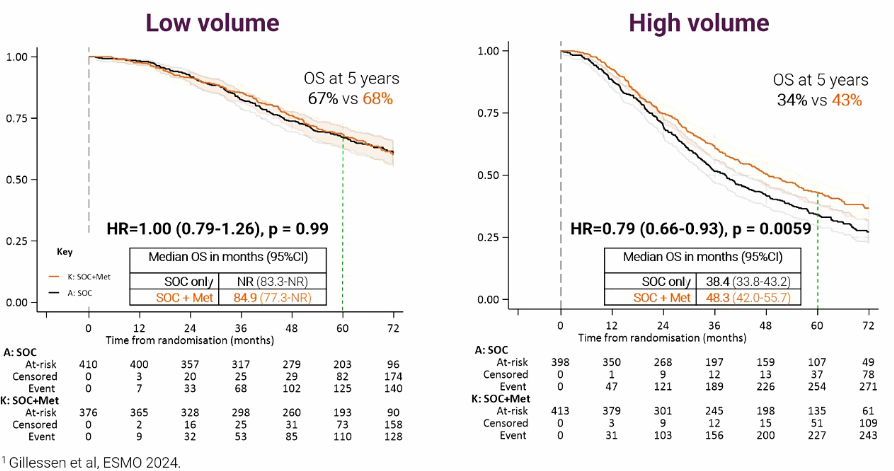
但我们在一项预先设定但并未依据统计效能所设计的亚组分析(依据转移负荷进行分层)发现,对于低容量转移患者,二甲双胍并无生存获益(HR 1.0);而对于高容量转移患者(按照CHAARTED标准定义),联合二甲双胍治疗具有明显优势(HR 0.79),这意味着大约能够延长患者生存期近10个月。
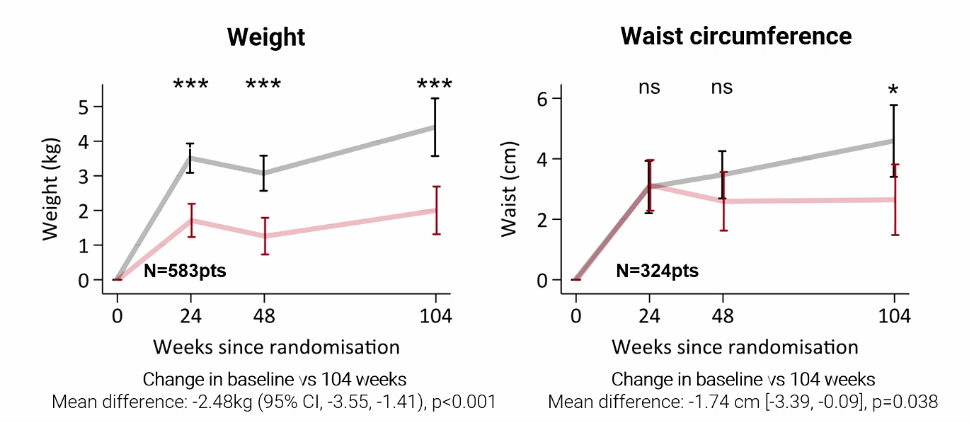
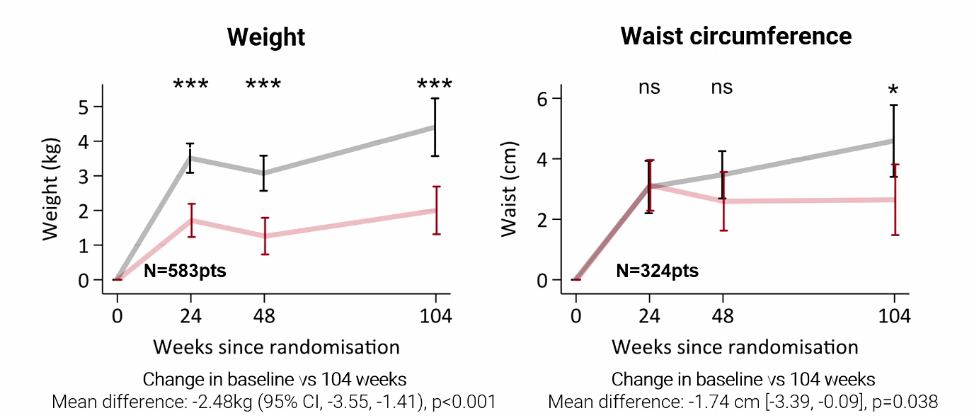
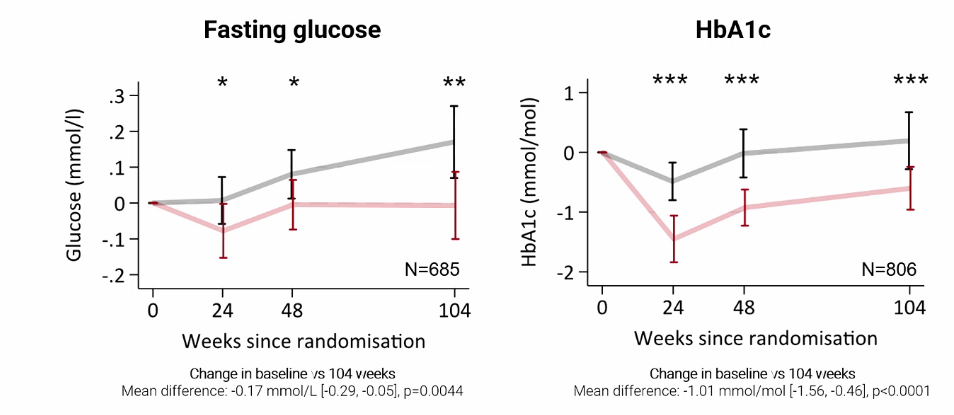
从代谢方面来看,二甲双胍的作用也非常显著。ADT治疗通常会引发体重增加、血糖异常以及血脂升高等一系列代谢问题。而在我们的研究中发现,接受二甲双胍联合治疗的患者在代谢副作用方面有明显改善。具体而言,在体重增加幅度方面,二甲双胍组仅为2.5 kg(vs 标准治疗 4 kg,P<0.001);腰围增加幅度也相对较小(P=0.038);血糖控制情况更为良好;总胆固醇和低密度脂蛋白(LDL)水平均更低。尤为值得关注的是,代谢综合征的发生率更低(4.9% vs 标准治疗组9.4%)。
综合上述各项研究结果来看,二甲双胍不仅有可能为高容量患者带来生存获益,而且能够显著缓解长期ADT治疗所导致的代谢副作用,这无疑为转移性激素敏感型前列腺癌患者的治疗提供了新的思路和方向。
UroStream:You shared the STAMPEDE study of metformin for mHSPC at the conference. What improvements has this combined treatment strategy brought to patients? What impact will it have on future clinical practice?
Dr. Ashwin Sachdeva:Yes, we presented new data from the STAMPEDE metformin trial, specifically focusing on patients with metastatic hormone-sensitive prostate cancer (M1). In this study, we enrolled approximately 1,800 patients who were randomized to receive either standard of care alone or standard of care combined with lifelong metformin for those with metastatic disease. The trial’s primary endpoint was overall survival, while a key secondary endpoint—also the focus of my presentation today—was the metabolic impact of adding metformin. The overall survival data, which we presented at ESMO last year, showed no statistically significant benefit across the unselected population, with a hazard ratio of 0.91.
However, when we performed a pre-specified (though not pre-powered) subgroup analysis based on metastatic disease burden, we observed a nuanced pattern. In patients with low-volume disease, metformin did not confer any added survival benefit (HR 1.0). But among those with high-volume disease, as defined by the CHAARTED criteria, the addition of metformin showed a meaningful benefit—an estimated hazard ratio of 0.79—which corresponds to an approximate 10-month improvement in overall survival. These are the patients with more aggressive disease, and this subgroup appears to derive the most benefit.
Today, I presented the trial’s findings on metabolic outcomes, which are particularly relevant because, as mentioned earlier, ADT increases the risk of cardiovascular complications, diabetes, weight gain, and lipid abnormalities. We found that metformin reduced many of these side effects. For instance, weight gain was significantly less in the metformin group—on average, 2.5 kg compared to 4 kg in the standard of care group. Increases in waist circumference were also smaller in patients receiving metformin. We also saw improvements in glycemic control, total cholesterol, and LDL levels. Perhaps most notably, the incidence of metabolic syndrome—a major concern in patients on long-term ADT—was nearly halved: 9.4% in the standard of care arm versus only 4.9% in the metformin arm.
Altogether, these findings suggest that adding metformin to standard treatment not only has potential survival benefits in high-volume metastatic patients, but also meaningfully reduces the metabolic side effects commonly seen with prolonged ADT.
Ashwin Sachdeva:确实,在STAMPEDE试验中,大约85%患者的标准治疗方案为ADT联合多西他赛。然而,受疫情影响而暂停招募后,标准治疗方案发生了变更,新增了ARPI,因此仅有约50名患者在使用二甲双胍的同时,接受了ADT联合ARPI治疗。由于样本量有限,我们暂时还无法就该组合给出确切的疗效结论。因此有必要进一步扩大样本量,纳入更多患者进行研究。
不过可以明确的是,长期ADT的副作用已十分明确。即便ADT联合ARPI应用,ADT所引发的代谢毒性依然存在,甚至可能出现毒性增强的情况。尽管当前尚未有确切的数据表明二甲双胍能够缓解ARPI带来的额外毒性,但我们有充分的理由相信,它能够持续减轻长期ADT治疗所导致的代谢副作用。基于目前的研究结果,我们建议临床医生在运用ADT时,可考虑联合使用二甲双胍,从而更有效地控制长期副作用,为患者带来更大的临床获益。
UroStream:Currently, ADT+ARPI has become an important treatment option for mHSPC, but the number of patients included in the study is relatively small. What do you think of the efficacy of metformin combined with ARPI+ADT?
Dr. Ashwin Sachdeva:Yes, you're absolutely right. In the STAMPEDE metformin trial, about 85% of enrolled patients received standard of care consisting of ADT plus docetaxel. However, after a recruitment pause during the COVID-19 pandemic, the standard of care evolved to include ADT plus an ARPI agent. As a result, only around 50 to 54 patients in the metformin arm received this newer treatment combination.
In terms of what this means for clinical interpretation, the sample size for the ADT+ARPI subgroup is currently too small to draw definitive conclusions. The only way to obtain robust evidence would be to continue the trial and recruit a larger number of patients receiving ADT+ARPI.
That said, we can take comfort in what we already know: the long-term side effect profile of ADT is well established. Even when combined with an ARPI—forming a doublet backbone—the adverse effects of ADT, such as metabolic disturbances, persist and may even be amplified.
Although we don’t yet have clear data on whether metformin can directly mitigate ARPI-related side effects, we are confident that it continues to help reduce the adverse effects associated with long-term ADT alone. So based on the data presented today, I would encourage clinicians to consider starting patients on metformin, particularly those undergoing prolonged ADT, to better manage and reduce long-term toxicities.
参考文献:
Sachdeva A., et al. A0516: Metabolic benefits of adding metformin to androgen deprivation therapy for patients with metastatic Hormone-Sensitive Prostate Cancer (mHSPC): Results from the STAMPEDE metformin trial. EAU 2025
Ashwin Sachdeva
英国曼彻斯特大学
泌尿外科临床高级讲师,癌症科学系
(来源:《肿瘤瞭望-泌尿时讯》编辑部)
声 明
凡署名原创的文章版权属《肿瘤瞭望-泌尿时讯》所有,欢迎分享、转载(开白可后台留言)。本文仅供医疗卫生专业人士了解最新医药资讯参考使用,不代表本平台观点。该等信息不能以任何方式取代专业的医疗指导,也不应被视为诊疗建议,如果该信息被用于资讯以外的目的,本站及作者不承担相关责任。
温馨提示
添加小助手请备注“泌尿”